What the DSM and Its Replacements Keep Missing
Every experienced clinician eventually hits the same wall. You’re sitting with a brain map on one screen and a diagnostic label on the other, and they don’t match. Not in the way that ambiguous data doesn’t match—in the way that the label seems to be describing a different reality than the map.
Two clients, both carrying an ADHD diagnosis. One shows the classic pattern—excess frontal theta, a system that can’t hold a configuration long enough to do anything with it. The other shows rigid alpha dominance, locked so tight it can’t shift gears at all.
Same label. Opposite architectures. Hand them the same prescription and one might improve while the other gets worse—not because medication doesn’t work, but because the category can’t tell you which architecture you’re treating.
This isn’t a boundary issue. It’s not that we drew the lines in the wrong places. It’s that we’re drawing lines on the wrong surface entirely.
Better maps of the same territory
The field knows this. That’s why alternatives keep emerging.
The NIMH’s Research Domain Criteria—RDoC—reorganizes mental illness around brain circuits and functional domains instead of symptom checklists. Dimensional instead of categorical. Multi-level instead of surface-only. A genuine improvement.
HiTOP, the Hierarchical Taxonomy of Psychopathology, takes a data-driven approach, organizing psychopathology by statistical co-occurrence rather than committee consensus. It captures comorbidity naturally, because it’s built from the patterns themselves rather than imposed on top of them.
And Denny Borsboom’s network theory goes further still, proposing that disorders aren’t hidden entities behind symptoms but emergent patterns of symptoms—feedback loops that get stuck. Disorders as attractor states. That’s a real insight.
Each of these frameworks is smarter than the DSM. Each one captures something the DSM misses. And each one is still operating at the level of what appears.
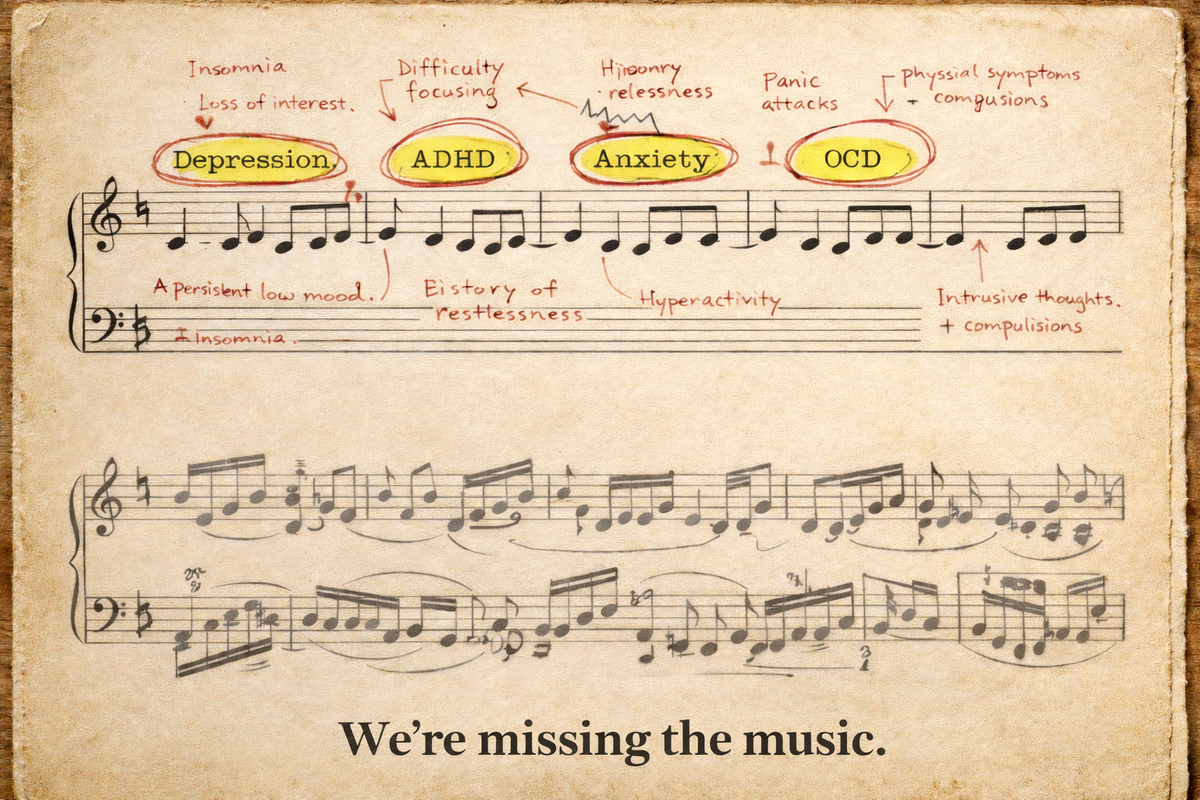
RDoC organizes appearances by circuit. HiTOP organizes appearances by co-occurrence. Network theory maps how appearances sustain each other. Better cartography, genuinely. But still cartography of the surface. Still the lyrics of the song, analyzed with increasing sophistication—when the problem might be in the score.
At a certain point, rearranging descriptions of what distress looks like stops producing new understanding. You can reorganize symptoms dimensionally, hierarchically, causally—and still never touch the question underneath: why does thinking break down in these ways and not others?
That question requires a different kind of looking.
A different way of seeing
There’s an old myth that gets at this more precisely than any methodology paper.
Perseus was sent to kill Medusa—the creature whose direct gaze turned men to stone. He couldn’t face her. Everyone who tried was destroyed by what they saw. His solution wasn’t a better weapon. It was a different way of seeing. He used the polished surface of his shield as a mirror, engaging the threat through its reflection rather than its appearance.
The shield was a gift from Athena. Goddess of wisdom. Goddess of strategic reason. That’s not incidental. The myth encodes a structural insight: some problems cannot be solved by looking harder at what presents itself. They require a reflective surface—a way of seeing the pattern rather than being overwhelmed by the content.
This is precisely the situation psychology faces with the DSM and its successors. Symptoms are Medusa’s face. Look at them directly—catalogue them, cluster them, map their causal interactions—and you’ll produce increasingly detailed descriptions of what overwhelms. But the descriptions themselves won’t explain why the mind organizes distress this way. For that, we need to stop looking at what appears and start looking at the structure that produces what appears.
In the language I’ve been developing across my clinical and philosophical work, this is the difference between semantics and syntax. Semantics is content—what thoughts are about, what experiences feel like, what symptoms look like from outside. Syntax is structure—how elements are organized so that meaning, experience, and yes, dysfunction can arise at all.
We’ve been studying the semantics of distress. What we need is the syntax of thought.
The lineage of an audacious idea
I want to be honest about the scale of this claim. To say that we can understand the structure of human thought—not its content but its architecture, the grammar that makes thinking possible and the specific ways that grammar can deform—is among the most ambitious statements anyone in this field can make. It should be scrutinized. It should invite skepticism.
But it doesn’t come from nowhere. And it doesn’t come from just me.
Gottfried Leibniz, three centuries ago, envisioned what he called a characteristica universalis—a formal language of reasoning itself. Not a language for describing what we think about, but for capturing how thinking works. He didn’t finish it. No one has. But the ambition was structurally precise: thought has a grammar, and that grammar can in principle be made explicit.
Karl Pribram, the neuroscientist, approached a related question from the other direction. In Languages of the Brain, he asked what form information takes in the nervous system beforesymbols emerge—before words, images, or concepts. What he found was distributed, phase-sensitive, relational—a language of timing and interference, not of labels and locations. Meaning, in his account, isn’t stored like a file. It’s assembled, the way an image emerges from overlapping waves.
Carl Jung was mapping something similar from the inside. His archetypes and complexes were never meant as literal entities—they were structural regularities in how the psyche organizes itself. Attractors, in everything but name. Stable configurations that shape what a mind can do and where it gets stuck. He used mythology because that was the descriptive language available to him. The underlying observation was structural.
My own work builds on this entire lineage. The questions that drive it go back nearly twenty-five years—a curiosity about the structure of thought that began long before I had any clinical tools to test it. That curiosity eventually led me to neurotherapy, where for the first time I could see organizational dynamics expressed in real physiology, in real people, in real time.
The formal framework I’ve developed across that arc—and laid out in my upcoming book The Quantified Soul—isn’t new in its ambition. What’s new is the convergence. We now have instruments precise enough to read the expression of thought’s organization through physiology, and formal frameworks rigorous enough to describe what we’re reading. The bridge that Leibniz imagined and Pribram began to build can now be walked across. Not just philosophically—clinically.
The instrument and the music
But a crucial clarification has to be made here, because this is where most attempts at mind-brain integration go wrong.
What we observe in EEG—the spectral dynamics, the phase relationships, the event-related potentials—is not thought itself. It is thought’s expression, filtered through biology, constrained by genetics, shaped by development, mediated by neurochemistry and anatomy and everything else that embodiment entails.
The brain is not the mind. The map is not the territory. But in a framework where physical and mental reality are understood as correlated expressions of the same underlying organization—two aspects of one thing, not two separate things—the physiological signal becomes structurally informative even though it isn’t identical to the mental reality it expresses.
Think of it this way. The same song can be played on piano, guitar, or voice. The instrument shapes the sound—its timbre, its range, its texture. But the music—the pattern of relationships between notes, the phrase structure, the resolution and tension—persists across instruments. If you understand music theory, you can hear the structure through any instrument, even a poor one.
The brain is the instrument. The mind is the music. What we read in EEG is the instrument’s behavior. But because the instrument is playingsomething—because the physiological dynamics aren’t random but are expressions of an underlying organizational pattern—we can learn to hear the music through the measurement.
And here’s what makes this clinically explosive rather than merely philosophically interesting: if we shape the expression, we influence the thinking. Not metaphorically. That is literally what neurofeedback does.
When you train a brain toward more flexible dynamics, the person doesn’t just show better numbers on a screen—they report thinking differently. When you help a rigid system release a configuration it’s been locked into, the person doesn’t just look calmer in the data—they experience a shift in how possibility feels.
The expression and the thought move together, because they were never separate. Two faces of the same organization—and you can reach one through the other.
Systems don’t get depressed
This brings us back to the clinical room—and to the question the DSM was always trying to answer, with the wrong tools.
Does a system get depressed? No. Depression is a word we apply to an experience.
But a system can fail to mobilize adequate resources when demand increases. It can lose the capacity to shift state, to generate the kind of reconfiguration that corresponds to engagement, motivation, the felt sense that action is possible and worthwhile.
When that organizational failure persists, the person living inside that system experiences flatness, heaviness, a draining of color and purpose—the things we call depression. The suffering is real. The experience is real. But the label is pointing at the surface, and the cause is structural.
Different structural failures can produce overlapping surfaces. A system that can’t recruit—can’t mobilize when life demands it—looks like depression. But so can a system that can’t release—one locked into a vigilance configuration that exhausts its resources, leaving nothing available for engagement. Same symptom picture. Same DSM code. Opposite organizational dynamics. Opposite treatment implications.
This is why the labels bleed into each other. This is why comorbidity is the rule rather than the exception. This is why two clients with the same diagnosis can need interventions that are not just different but contradictory. The categories were built from appearances, and appearances underdetermine structure. Same lyrics, different score—and the score is where the information lives.
A structural vocabulary—one that describes how organization fails rather than what failure looks like—changes what’s possible in the room. It tells you not just that someone is struggling, but what kind of reorganization their system actually needs.
I’ll unpack that vocabulary in a future essay: the finite set of ways a system’s coordination can break down, each with its own signature, its own clinical implications, its own path toward restored flexibility. Not a new set of labels to replace the old ones.
A grammar of organizational failure—a syntax of how minds come apart and, sometimes, find their way back.
Reading the score
This is not just a better diagnostic framework. It’s a different relationship to the mind entirely.
The DSM gave clinicians a shared vocabulary, and that mattered. The alternatives are giving us better statistics, better dimensions, better maps. What’s still missing is understanding—the ability to see how a particular system is organized, where that organization is breaking down, and what kind of structural shift would restore the flexibility the system has lost. That requires reading at the level of syntax, not semantics. Score, not lyrics. Pattern, not appearance.
The clinician who can do this isn’t applying labels. They’re reading structure. And the mind being read—if the framework holds—is not a black box generating mysterious outputs, but an organization whose dynamics can be seen, described, and in many cases, helped to change.
That’s the project. Not to explain the mind away, but to finally learn to read how it holds together, how it comes apart, and what it needs in order to find its way back into form.
Comments ()